Leave a Comment:
(0) comments
Add Your Reply


The CDC is very much in line with the WHO in what it endorses. If the WHO approves of something, you can count on the CDC to pretty much follow their lead.
But the CDC would prefer that you not look too closely at what they publish. They’d rather you just take their word for it through the lenses of their “unbiased experts” like Anthony Fauci.
However, when you take the time to look at their facts more carefully, what you find are trails leading to what is likely to end up, when all is said and done, to be one huge deceptive lie.
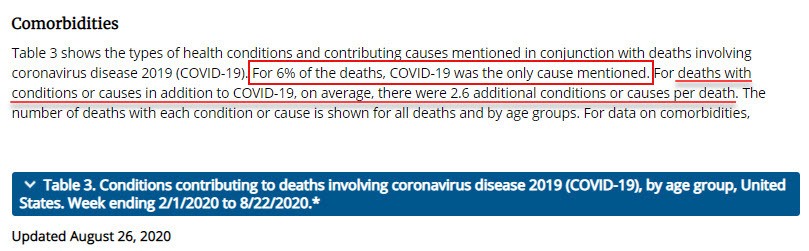
Recently, information was released that revealed that the CDC only acknowledges 6% of the COVID mortalities reported were caused by the SARS-CoV-2 virus alone. The other 94% were for deaths with conditions or causes (called comorbidities) other than the COVID-19 virus.
FB and other Big Tech media immediately jumped into the breach and claimed that anyone who claimed that only 6% of the deaths from the CDC numbers was false information. Why? Because the 94% who died from other causes were weakened by those other morbidities, which allowed the COVID-19 virus to finish them off.
Despite Big Tech’s protective claim, this is certainly not false information as you can see below. Nor has the conclusion proven to be false.
They may be attempting to insert another interpretation of the conclusion, to save the face of the pandemic panic narrative, but the fact is, this is based on what the CDC actually stated on its website.
One clearly sees from the screenshot below that the CDC’s assertion. As the screenshot clearly shows in reference to its Table 3, only 6% of deaths were directly attributed to the COVID virus.
The remaining 94% were:
For deaths with conditions or causes in addition to COVID-19, on average, there were 2.6 additional conditions or causes per death.
Let’s first flesh out those figures a bit using data that the CDC provides in table 3 on its site when I made the screenshot:
Facebook’s fact-checkers took issue with the conclusion that just because they died with comorbidities doesn’t mean that SARS-CoV-2 (called COVID-19) was not the primary cause of death.
Another line of argument they advanced is that the COVID-19 virus could have caused those other morbidities.
Did they provide any evidence to confirm that claim? Nope! It was just a claim by an “expert” fact-checker.
However, the other morbidities are of a nature that they do not develop quickly as does the alleged virus. These are diseases that take years, even decades, and additionally, often involve long term treatment with pharmaceuticals as well.
To claim that these comorbidities arose because of a short term virus is not a sensible conclusion, especially considering the groups’ age in question.
More sensible to me would be to conclude that people with pre-existing diseases, who are also physically older, are more susceptible to contracting viruses and bacteria. (If you accept that a virus can only arise by contagion, which I believe along with others, is not the case.)
However, based on CDC tables, let’s flesh out the COVID-19 mortalities a bit further to see if this COVID disease-producing claim makes sense.
According to the CDC in its Table 3 totals:
In other words, most so-called COVID deaths were aged citizens with over two morbid health conditions or more.
Conditions like:
Claiming that these pre-existing diseases (comorbidities) arose from the virus does not fit with these disorders’ long-term nature.
Perhaps, it made them more susceptible to the virus as previously stated, but to assume that a short-term event produced a long-term disease is clearly putting the cart before the horse.
Where are the “facts” to confirm the fact-checkers claim? Much like the anonymous sources of President Trump’s alleged accusers, they never appear. I don’t think we have to wonder too much as to why that is the case.
However, it does beg some questions in my mind like:
Nevertheless, the most critical factor of all to look at with these assumed cases is how they were categorized as a COVID case in the first place:
The question never examined nor brought up by any of the media, politicians, and quite frankly, most people these days is the test’s integrity.
Everyone in the media, even the so-called conservatives, accepts the CDC COVID-19 mortality figures as factual – without question.
But, are these mortality figures as accurate as we are all led to believe?
That assumption is very questionable if you take a little time to look at what the CDC has to say about the test.
Based on what the CDC says its guideline booklet to the RT-PCR test for professionals, the test is not all that accurate or definitive.
The CDC notes in its guidelines to the test CDC 2019-Novel Coronavirus (2019-nCoV) Real-Time RT-PCR Diagnostic Panel:
Positive results are indicative of active infection with 2019-nCoV but do not rule out bacterial infection or co-infection with other viruses. The agent detected may not be the definite cause of disease. Laboratories within the United States and its territories must report all positive results to the appropriate public health authorities.
Negative results do not preclude 2019-nCoV infection and should not be used as the sole basis for treatment or other patient management decisions. Negative results must be combined with clinical observations, patient history, and epidemiological information.
Translation: A positive test may result from a bacteria (which is 100x larger than a virus and considered a living entity which has mobility and a means of digestion, unlike a virus.) or other viruses.
That leaves a pretty wide swath of other organisms which can generate a positive RT-PCR result, doesn’t it?
Additionally, even though positive tests may be caused by a living entity like a bacteria (which we all have and need btw to do important things like digest our food and rid the body of dead cells) or another virus, the testing entity must report it to the “appropriate health authorities.”
I wonder if those unreported facts jack up the COVID mortality figures and overall numbers with false positives? It doesn’t take a medical expert or fact-checker to answer that question.
This unacknowledged excerpt is a little-known but significant fact that brings RT-PCR test results very much into question. What we learn from this fact is that a completely different organism like bacteria, or even other viruses, can cause a positive COVID test result.
Since, as noted above, we all possess bacteria to digest our food and help rid the body of dead cellular matter, wouldn’t this mean that just about any of us could test positive for the RT-PCR test?
Another factoid: Bacteria are the most populous living organism on the planet. Although, a newly discovered virus may displace it.
Factoid: The genome of our internal bacteria alone far exceeds our own human genome. According to an article on the site Big Think, we are 10% human and 90% microbial!
Additionally, we also have viruses other than the SARS-CoV-2 virus in our bodies which also serve a functionally necessary purpose. Could not these “other viruses” also cause a positive test result?

Yet, all positive tests must be reported to the appropriate health authorities, according to the CDC.
Therefore, how can we be sure that the 94% group who have co-morbidities, which weakened them to the COVID virus’s impact, really do have the SARS-CoV-2 virus?
As the CDC acknowledges, the positive test could be the consequence of live bacteria or even another virus. How do we know it wasn’t?
Hint: We don’t because…ALL positive tests must be reported: “to the appropriate health authorities .” That would be, of course, be the CDC.
These facts, which are never shared with the public, make the test results questionable, at best. All of them. Not just some of them.
The inventor of the RT-PCR test- Kary Mullis, states that the test can not be used for diagnostic purposes because “with PCR you can find almost anything in anybody.” Hence, the test is meaningless as a diagnostic tool.
Even the WHO has recently admitted that released a guidance memo on December 14, 2020, warning that high cycle thresholds on PCR tests will result in false positives. The PCR test works by amplifying a sample or doubling the contents of the sample to produce greater amounts that can be used for analysis. Each cycle is called a Ct cycle.
The higher the Ct value or number of cycles, the less likely you are to be detecting anything significant. A heavily infected person would demonstrate large amounts of an infectious agent with relatively few cycles.
Additionally, the more cycles or Ct’s run, the more likely the test will generate false positives. More on that below. The WHO memo states:
The design principle of RT-PCR means that for patients with high levels of circulating virus (viral load), relatively few cycles will be needed to detect the virus and so the Ct value will be low. Conversely, when specimens return a high Ct value, it means that many cycles were required to detect the virus. In some circumstances, the distinction between background noise and the actual presence of the target virus is difficult to ascertain.
WHO (finally) Admits PCR Tests Create False Positives
The largest manufacturer of the test (Roche) also agrees with Mullis in their package insert which states quite plainly – “This test is not to be used for diagnostic purposes”. Watch below:
Another important aspect to understand is how they produce their results. The RT-PCR test works through amplification. The RT stands for reverse transcription which means that through the polymerase enzyme chain reaction it turns RNA into DNA.
You take a small sample and keep “amplifying” it. That is, you make the sample larger and larger, by making copies of it. Two becomes four, four becomes eight and so on. A standard cycle is 35 times.
As new copies of the viral DNA sections are built, the marker labels attach to the DNA strands and then release a fluorescent dye, which is measured by the machine’s computer and presented in real time on the screen.
How is the COVID-19 Virus Detected Using Real Time RT-PCR?
The computer tracks the amount of fluorescence in the sample after each cycle. When a certain level of fluorescence is surpassed, this confirms that the virus is present.
Scientists also monitor how many cycles it takes to reach this level in order to estimate the severity of the infection: the fewer the cycles, the more severe the viral infection is.
Here’s the problem with that. Confirmation of a match does not mean the person has any level of the match (allegedly the virus) that poses such a threat to the person that it will overwhelm their immune system. The test doesn’t tell you anything about how much of the assumed virus is in the person’s body!
They can assume the level if it shows up sooner in the cycle process, but that doesn’t confirm it, nor does it confirm that the person’s immune system cannot easily overcome the assumed virus. We all carry viruses and bacteria in our bodies. If the microorganism is a threat, it must be present in numbers large enough to be indicative of a problem in that person’s internal condition.
The PCR test says nothing about that important factor at all. It simply confirms that some snippet of the persons internal RNA code matches the assumed SARS-CoV-2 virus. The questionable assumption is that the presence of a test match means the person is infectious and therefore dangerous to everyone around them.
Hint: There isn’t any.
All of us carry viruses and bacteria around in our bodies, as previously noted. The fact that an amplified snippet of DNA matches the assumed SARS-CoV-2 virus DNA (which from what I understand has never really been isolated and proven in a lab) does not mean that the person is under threat of getting ill from the match.
This is why so many people, even if they do test positive, have no symptoms from the allegedly fatal virus. Even if present, which is questionable since they have never really isolated the virus in the first place, their immune system easily overcomes the amount that may be circulating in their body. Hence, no symptoms and thus no threat nor treatment needed.
In fact, the treatments are proving to be worse than the virus.
According to Web MD, a study of 5,700 COVID-19 patients hospitalized between March 1 and April 4, 2020, at Northwell Health, New York State’s largest health system, deaths of those on ventilators rose to 88%.
That is, nearly all COVID-19 patients died after being placed on a ventilator. Obviously, the ventilator is not working as a method of saving lives.
Of course, the spin from the hospitals and media is that ventilators saved 12% of the people who used them who otherwise would have died. So. we’re back to the assumption game once again. Personally, as a patient, the statistical odds would not encourage me to select the ventilator as a means of survival. As we shall see below however, there is another incentive to put the patient on a ventilator outside of the life saving potentials that may be impacting the choice of treatment.
Then, we have another issue. The accuracy of the tests.
According to a podcast on This Week In Virology (TWiV) on July 17, 2020, Dr. Anthony Fauci stated that an RT-PCR test with amplification cycles above 35 are practically worthless and misleading:
“…If you get [perform the test at] a cycle threshold of 35 or more…the chances of it being replication-confident [aka accurate] are miniscule…you almost never can culture virus [detect a true positive result] from a 37 threshold cycle…even 36…”
TWiV 641: COVID-19 with Dr. Anthony Fauci (beginning at around the 5 minute mark)
Each test is a quantum leap in magnification of the original patient test specimen which is to say each cycle doubles the amount of DNA or RNA in the sample. You are just multiplying the strands with each cycle.
What the PCR test does not do is generate quantitative results. As previously noted, it does not tell you how much of the RNA or DNA match exists in the bloodstream or how much of a viral load the person has. It simply tells you it is present.
You may only have a minuscule amount of a matching DNA/RNA and likely do because we all carry viruses inside of our bodies which act as a clean-up and detoxification agent. A viral load which is perfectly normal and necessary for our health.
If you amplify (run enough cycles of the test), you increase your chances of finding the match you are seeking exponentially. Conversely, if you run less cycles you are likely to find no match, unless there is a very large quantity in the nasal passage from where the PCR sample is drawn from.
What Fauci failed to say during the podcast however is that the FDA, which authorizes the test for the public, recommends the test be run for 40 cycles, NOT 35. This increases the chances of generating many useless false positives by detecting minuscule amounts of the matching RNA. Healthy people with a nominal amount of the virus will have no negative impact upon their health.
These would be the healthy people (like athletes) who tested positive but have absolutely no symptoms or are asymptomatic (without symptoms). Yet, the case numbers go up anyway because the test generated a positive. Meaningless, without impact, but a positive result and another number to add to the COVID case count.
The video below explains the misinformation produced from the RT-qPCR tests as the amplification threshold is advanced:
[youtube_advanced url=”https://www.youtube.com/watch?v=S_1Z8cSXI-Q” controls=”no” rel=”no” theme=”light”]The labs in the U.S. that follow the FDA guidelines are either knowingly or unknowingly participating in the generation of false positives. Millions of Americans are being told they are infected with the COVID virus on the basis of a false positive result.
All these lockdowns and mask mandates based on the false numbers being generated are based on an illusion. The COVID19 totals, based on this test, are grossly false. As suggested in the video above and even in the CDC’s testing guidelines, the test was never meant to be the sole determinant of whether a person had the SARS-CoV-2 virus and was infectious.
Yet, that is what is happening all over the planet and in the United States. The test is being used as the sole determining factor of whether someone has the virus or not.
The left-leaning NY Times even confirms the assumptions above with a little test of its own.
The New York Times reviewed PCR test data compiled by officials in Massachusetts, New York, and Nevada.
They discovered that up to 90% of those testing positive either carried no virus or such a small amount as to be of no danger whatsoever.
Ninety percent! That is 9 out of 10 cases. How many of those tests became cases in the COVID-19 case count numbers one must wonder?
Hint: All of them.
If you have followed along here, you can see there are a number of factors that will generate false numbers adding fear mongering ammunition for those who wish to use these numbers to generate more control and power over citizens like politicians or simply more income for their hospital as you will see below.
This isn’t complicated or difficult to understand. In fact, it is quite simple:
Perhaps that is the real reason for the increased testing emphasis. Not public safety, because it isn’t difficult to discover that testing should not be the primary determinant. Rather, more control over the public by generating growing case numbers even if they are based on inaccurate data.
They can keep the public in line with the growing reporting of all of those scary new cases even if they are based on false positives or artifacts resembling the so-called virus that have absolutely no infectious threat.
Which brings us to another important consideration:
Buried on page 39 of the RT-PCR test manual is the following:
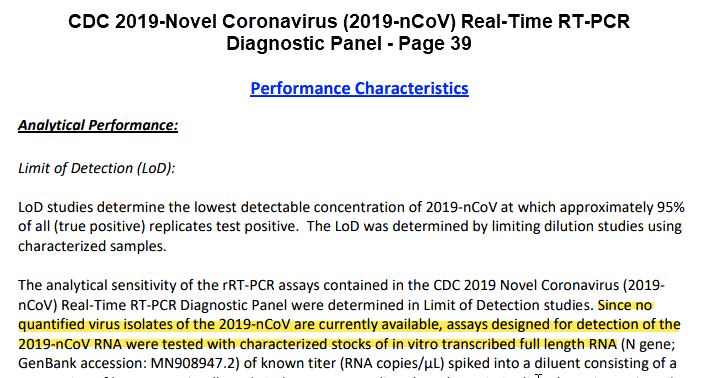
The key phrase therein is:
Since no quantified virus isolates of the 2019-n-CoV are currently available…
RT-PCR Manual p. 39
The phrase “quantified” means measurable. “Isolates” means no COVID-19 SARS-CoV-2 was isolated and available to test.
This begs the question then that if no measurable isolates of SARS-CoV-2 were available what exactly was used to test for the virus?
The answer is that the SARS-CoV-2 was never properly isolated for testing. Thus, it was never properly proven to exist. They used stocks they assumed were similar to what they thought the COVID-19 virus was for the RT-PCR test, not the actual virus. Is an assumption good enough to base a global lockdown and mandatory mask mandate upon?
Is that supposed to be scientific? Uh, it ain’t. At least not in standard, textbook based scientific circles.
It’s kind of like saying, I did my homework, but the dog ate it or the money for the mortgage is in the bank, when you don’t have it to make the payment and never did. How can you base a test on a virus that has not been properly isolated and made available?
This begs another important question.
The answer? We can’t. These tests not only demonstrate positives for bacteria and other viruses, but they also never had the claimed virus to test with in the first place.
If you are wondering why this seems to have developed into a political rather than a health-related deadly viral pandemic, you needn’t wonder any more. It always was.
But wait, there are other fudge factors built into this COVID equation – the COVID-19 categories.
FOIA requests were submitted 6 months ago by Christine Massey, a Canadian citizen, asking for proof that the SARS-CoV-2 virus has been isolated. So far, 40 agencies worldwide, including the Public Health Agency of Canada have responded with no proof of isolation.
Massey’s responses can be found at this page: https://bit.ly/3nQurs8
There are two categories used to classify a case as a COVID case.
One is the confirmed category, which means the patient meets the confirmatory laboratory evidence for COVID-19.
As you have just seen, if the confirmed case basis is a positive RT-PCR (reverse transcriptase-polymerase chain reaction) test, a confirmed case is not as “confirmed” as we are led to believe.
However, suppose we leave that as it is and consider the second category – the probable and presumed case category.
COVID-19 deaths are identified using a new ICD–10 code. When COVID-19 is reported as a cause of death – or when it is listed as a “probable” or “presumed” cause — the death is coded as U07.1. This can include cases with or without laboratory confirmation.
COVID-19 Death Data and Resources
I’m sure, with a little reflection, you can see the problem with this category,
Probable and presumed cases require no confirmatory laboratory testing. None!
A potential case only has to meet a presumption of laboratory evidence and clinical criteria or epidemiologic evidence, which means the assumed symptoms of the COVID-19 disease complex.
A patient doesn’t even need a confirmed test to be considered a COVID case. All the patient needs are symptoms (which keep expanding) connected with COVID-19, and they fall into the probable COVID case category.
According to the CDC’s Guidance for Certifying Deaths Due to Coronavirus Disease 2019 (COVID–19) from their Vital Statistics Reporting Guidance which is still used:
In cases where a definite diagnosis of COVID–19 cannot be made, but it is suspected or likely (e.g., the circumstances are compelling within a reasonable degree of certainty), it is acceptable to report COVID–19 on a death certificate as “probable” or “presumed.”
Report No. 3 ▪ April 2020
In these instances, certifiers should use their best clinical judgement in determining if a COVID–19 infection was likely. However, please note that testing for COVID–19 should be conducted whenever possible.
One wonders just how many of these “clinical judgement” calls end up in the COVID-19 number counts.
Of course, this is an easy way to add to the COVID numbers. Simply assume, based upon symptoms, that the case has been caused by the SARS-CoV-2 virus.
This begs another question.
With this liberal criterion, one can see how easy it could be to categorize a case as COVID-19. So:
As it turns out, when the lockdowns began, there was a great deal of hyperbole about how 2.5 million Americans would die as a result of the pandemic.
The projection was that hospitals would be overwhelmed and needed all the bed space they could muster to treat the COVID cases. Consequently, all elective surgeries (scheduled surgeries like hip and knee replacements, etc.) were forbidden.
For hospitals, that was devastating to the bottom line. For many hospitals, elective surgeries comprise up to 80% of their income. Predictably, hospital incomes plummeted, forcing lay-offs, and even closures for rural hospitals.
But there was an out provided to hospitals by Medicare/Medicaid, which constitutes most hospital patients since the aging population is the largest segment. This patient segment is a fact of life, not a condemnation. The body wears out over time.
As it turns out:
The video below by a doctor with 35 years of experience relates these facts:
So, you can see how there is an incentive built into this pandemic to categorize patients as COVID. The incentive, by the way, is paid for by the taxpayer.
You can also see how there are problems with the COVID numbers with the facts left out of the “fact-checkers” false information labeling. Labels that Facebook liberally pastes on any post that does not fully comply with the CDC narrative and numbers.
Yes, the fact-checkers of Big Tech and our media, politicians, and medical “experts” are all leaving out important information we are all entitled to know. Information that permits them to liberally adjust the COVID numbers and continue this power-producing and lucrative for some segments game of fear-based manipulation.
While ignoring all of these facts, truthful information gets tossed aside as conspiratorial – a common technigue used by the left to dismiss an opponent.
Could the real motive be that power-hungry Democrat politicians are happy to readily promote all reporting that feeds their narrative of controlling the citizens and denigrating the current President?
Why rock the boat with clarity when they can use the “cases” as scare tactics to justify oppressing the citizens of their states and cities?
Citizens decided to attend the Sturgis Biker’s rally because Krisy Noem, a Republican governor, was not locking down the citizens of her state, North Dakota.
Sturgis was a way for citizens to express their natural right to assemble peacefully by choice. The government and medical experts surely can’t allow that expression of freedom. Why that may just blow up their game of we own your life, for your own good, of course.

Why people may get the idea that there is nothing to fear here beyond the fear they generate. So, what happened?
A report quickly surfaces that “Houston, we have a problem!”
A study was published by the Institute of Labor Economics and conducted by economists at the University of San Diego who studied the Sturgis Motorcycle Rally.
Using data from the Centers for Disease Control and Prevention (CDC), the researchers then showed that a month following the rally, cases in the county where Sturgis is located rose by six or seven per 1,000.
US biker rally may have led to 260,000 new COVID-19 cases: study
Researchers said their calculations indicated “a total of 263,708 additional cases in these locations due to the Sturgis Motorcycle Rally”.
But wait, the article stated at the end:
A limitation of the study is that it was based on statistical methods, rather than tracking and surveying rally participants.
US biker rally may have led to 260,000 new COVID-19 cases: study
In other words, just like the predictions which came out of the Imperial College in the UK which started ALL of this pandemic panic, it was based on modeling projections, NOT facts! Like the Imperial College report, the numbers are inferred from assumptions, not reality.
However, there are other problems with this study as noted by a Forbes article. Like:
If you’ve read thus far, you’ll see that’s how the CDC rolls. Leave out the fine print and hype the assumptive conclusions. Conclusions based on fantasy and hype, not reality.
But let’s briefly look at the COVID reality.
Meanwhile, businesses have been put out of business – particularly small and medium-sized enterprises. No surprise there that small and medium are targeted in my mind.
Many people have been economically devastated. Some owners have lost businesses and employees have lost jobs that will never return.
Mental health issue have grown with a marked increase in suicides.
Children have been impacted in the family and in the normal educational pattern. (Of course, that actually may be beneficial in a number of ways but it does put a strain most particularly on lower-income parents.)
And there is a lot more. And probably more to come because once government gets its hook into something that controls the citizens, it is very, very difficult to remove that hook.
For those who have not bought fully into the COVID panic replete with the obligatory masks (which don’t work but that is another can of worms for another post), it is time for the people of these United States to get off this pandemic merry-go-round.
Let’s take off the masks. Interact face to face at normal civil distances and stop playing the COVID-19 pandemic panic game.
People want to get back to work. Politicians, mainly Democrats, would rather have them hiding at home “staying safe”. My guess is that it is probably to pin the failed economy on President Trump, as the media and Hiden Biden and Chameleon Harris are doing now when they do surface from time to time – an engineered absurdity like the riots in the Democratic-controlled cities.
People and businesses should begin to operate normally whether Democrat governors and Mayors tell them to or not.
Civil disobedience is being used by the left to push their agendas, like the violence allowed to run rampant in the Democratic controlled cities, now it is time to use it to push for our freedoms.
If enough people cast aside this falsely produced fear of what is essentially a “cold” virus, rely on common sense, including sensible nutrition, they can return to normal as soon as they choose.
Let the Big Tech fact-checkers on Facebook and censors on YouTube find another way to annoy the public. These so-called experts do not have all their facts straight and on the table anyway. Who cares what label they paste on a post or what video they ban?
As demonstrated, they are either willfully ignoring the facts or don’t even have them to work with in the first place. That is in no way an accident.
Our nation was founded on a Constitution of limited central government, but people are allowing a medical and media monopoly to scare them into enslavement based on fear tactics and a false pandemic.
Either we stop complying and start asserting our natural rights or we lose them forever. Keep this in mind when you select that next representative in the voting booth (if you are even permitted that in your state) from the President on down btw.
 COVID Hype and Dem Governor Tyranny Up – Mortality? Down
COVID Hype and Dem Governor Tyranny Up – Mortality? Down Completely Eliminated from the COVID-19 Panic – The Environment
Completely Eliminated from the COVID-19 Panic – The Environment Whatever Happened to the Concept of Free Market Health Care?
Whatever Happened to the Concept of Free Market Health Care? Illegal Immigrants Paid $4.2 Billion to Stay in U.S. Last Year with Bigger Tax Refunds than You.
Illegal Immigrants Paid $4.2 Billion to Stay in U.S. Last Year with Bigger Tax Refunds than You. Argentina’s Economy Still Struggling to Recover From Years of High Spending and Government Interventionism
Argentina’s Economy Still Struggling to Recover From Years of High Spending and Government Interventionism Another Thought on the 2nd Amendment- A Basic Truth Often Missing from the Discussion
Another Thought on the 2nd Amendment- A Basic Truth Often Missing from the DiscussionCOVID Hype and Dem Governor Tyranny Up – Mortality? Down
Completely Eliminated from the COVID-19 Panic – The Environment
The Scientist, Whose Doomsday Coronavirus Report Incited a Global Panic, Just Walked His Mortality Predictions Back to 4% of His Original Prediction
Do You Know What Is Really in the USMCA? Most Do Not
Fiona Hill’s Anti-Trump Connections Explains Why She Was On the Witness List
Vindman’s Odd Reaction During the Impeachment Sham
The Development of the Deep State – Part 1
Being An Ex-President Can Be Quite Lucrative As the Obama’s Demostrate